




Velma Scantlebury, who became the nation’s first black female transplant surgeon in 1989, believes there are more issues to overcome even after 30 years of achieving equity in organ allocation.
In a field dominated by white men and white surgeons, Scantlebury has had a tough time making her way in the realm of specialized surgery. But given her determination strong will and drive to achieve her goal, she only saw possibilities.
“My parents taught us that education is important and that we can be anything we want to be. I did not grow up seeing obstacles. I saw possibilities,” she told Zenger. “My parents knew I wanted to be a doctor, and despite not having any means, my mother came to the United States to clean floors … suffering much humiliation to bring us from Barbados to this country.
“She wanted to make it possible for me to become a doctor. So, with the strength and belief of my parents, my belief in God, and that all things are possible, I pursued my dream.”
As a result of the challenges she faced as a woman and as a woman of color in her profession, she wrote “Beyond Every Wall: Becoming the first Black Female Transplant Surgeon” for others who struggled with the same issues she did.
Today, she is a professor of surgery at Texas Christian University and the University of North Texas Health Science Center and Medical School, in Forth Worth, and a transplant consultant. In 2020, she retired from Christiana Care’s Kidney Transplant Program in Delaware.

Scantlebury has performed over 2,000 transplants and published peer-reviewed research papers. However, breaking barriers didn’t come easy. Being accepted as a colleague by white surgeons was difficult. Scantlebury was often excluded from social gatherings, likely, she thought, because they were uncomfortable around her.
“Racism was very evident. On a few occasions, patients objected to my being their surgeon. Only in one situation did the Japanese surgeon defend me and spoke up,” she said. Patients assumed I was there to clean their room, take their trays, but never the doctor. I had to maintain my self-esteem and keep telling myself, ‘Yes, I can! I am capable; I am talented, I can make it with the help of God.’
“It was not easy staying positive and strong,” she said. “The constant negativity took its toll, and after being a young mother, I found it difficult to be everything: wife, mother, surgeon, colleague, friend and deal with the rejection. At that time, I became depressed. I found it overwhelming because at that time, I watched my colleagues get promoted and be given leadership positions, and I was not getting the same treatment.”
When one of her South American colleagues admitted he was taking Prozac for his depression, Scantlebury realized she wasn’t alone, and it was OK for her to seek help. She also found a support system of friends and organizations who gave her a purpose and helped engage her outside of work.
While it was hard to deal with patients who felt uncomfortable with a black female surgeon, she soon realized it was their loss, not hers.
“When I was in training, there was not much I could do, especially when my leaders did nothing about it,” she said. “As a surgeon, I made sure I met as many patients before as possible, so they would not be surprised on the day of surgery. Otherwise, I told them I was the only choice, and they could pass on the organ transplant, and It will be given to someone else. That often changed their mind.” Scantlebury said.
In 1989, Scantlebury earned her Doctor of Surgery, but she had to pay a hefty price to get there.
“I feel that I paid the price of family. I had to be away at the hospital so much that I missed a lot of things with my children. As an adult, I now realize that my absence resulted in some emotional issues between them. I know I did the best I could with what little I knew. I lived away from my family, who was not there to help,” Scantlebury said.
Still, Scantlebury is content that her ground-breaking accomplishments as a transplant surgeon have opened a pathway for other women and women of color.
One time when she interviewed for a job in Alabama, she saw how pleasantly shocking it was for people of color to see her, a black woman, applying for the top position. It was more surprising for them to see Scantlebury arrive with braids in her hair — something she thought was appropriate and natural. Living in New York, this was acceptable, but in the South, it was a bold step at the time.
“This allowed other women to realize they could take that step also,” she said. “The silent rule was broken. I had stepped out and did something acceptable. Young girls look to me for possibilities. They, too, seek examples of what can be accomplished. I am glad to be that person,” Scantlebury said.
Dr. Sherry M. Wren, vice chair and professor of surgery at Stanford University, arrived at the University of Pittsburgh Medical Center the same time as Scantlebury, in 1989. Wren said she wishes she hadn’t seen the gulf between trainee and consultant as widely as she did.
“I was a transplantation research fellow, and she was a consultant surgeon on the transplant service,” Wren said. “I was in Pittsburgh from 1989-1994, and from 1992-1994, was a surgery chief resident. During that time, she was the only female transplant surgeon and one of two clinically active female surgeons in our residency program.
“It was inspiring to see two successful and talented women in a field that at that time had fewer than 5 percent women attendings (consultants). It wasn’t until years later I realized how close in age we were; she was an attending and therefore seemed so much further along than I was,” Wren said.
There are only 12 black female surgeons in the United States, but the pipeline is increasing, Many more are in training. Scantlebury expects these numbers to double in the next five years.

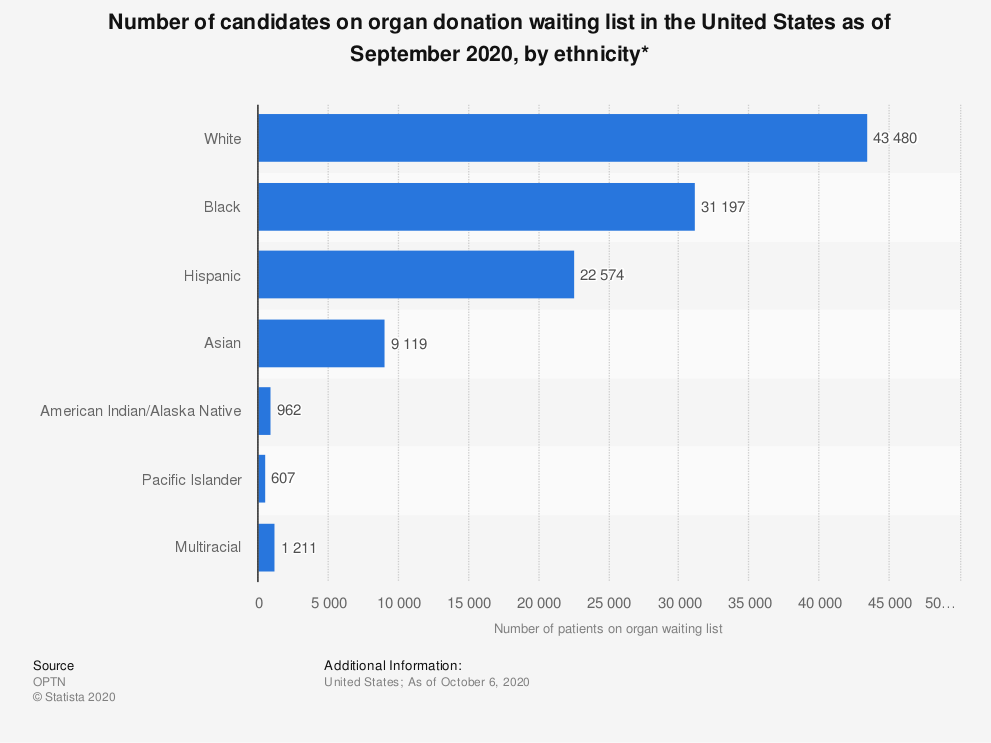
In addition to the shortage of black female surgeons, the lack of organ donors in the black community is at an alarmingly low rate. Scantlebury believes certain measures can increase awareness about the need for more organ donors among minorities.
One such organization trying to do that is the Minority Organ and Tissue Transplant Education Program founded in 1991.
African Americans have a more difficult time getting on kidney transplant lists, even though they are more likely to have end-stage renal disease. They have less access than whites to lifesaving kidney transplants. Scantlebury said some of the biggest challenges all black patients face include racism, achieving equity in health care, racism in medicine, poor treatment by doctors, lack of insurance, late referrals to specialists and health literacy.
“They are often diagnosed late, due to a lack of equity of health care. When referred to transplant, many have difficulty navigating the system to get the required tests. Hypertension and diabetes are more common in African-Americans, and despite this, many patients are neglected when it comes to getter their kidney function checked,” Scantlebury said.
“Being diagnosed in the late stage of renal failure happens more often than desired. My question to patients: ‘Who were you seeing? Were you going to your doctor?’ Usually, I hear: lack of insurance, could not afford the medications, doctor retired, could not go back as they owed money to the office, etc. Lack of health care for all is a problem in this country.
“Better education and more doctors being sensitive to the needs of patients — discussing options early and advocacy on the part of the doctors — can help,” Scantlebury said.
“For my part, I am working to bring equity to health care for the black community. Even after 30 years of achieving equity in organ allocation, issues persist. Education, advocacy, access, equitable care, action and empathy are key in achieving equity for access to transplantation.”
(Edited by Judith Isacoff and Fern Siegel)
The post Nation’s First Black Female Transplant Surgeon Advocates For Better Care For African Americans appeared first on Zenger News.





